
 Thyroid nodules are very common and a small percentage of these are malignant. Ask 10 thyroid specialists about their approach to biopsy and diagnosis and you will get 10 different approaches. All will be rational and based on reasonable scientific data and on experience. The different approaches arise because the research is varied in its recommendations. This partly arises because of the variable incidence of multinodular thyroids, variable incidence of malignancy, variable approach to reporting and imaging of thyroids, and different attitudes to how to deal with the many false positive and some false negative results that will arise more frequently the more biopsies are done. What is an acceptable level of inaccuracy?
Thyroid nodules are very common and a small percentage of these are malignant. Ask 10 thyroid specialists about their approach to biopsy and diagnosis and you will get 10 different approaches. All will be rational and based on reasonable scientific data and on experience. The different approaches arise because the research is varied in its recommendations. This partly arises because of the variable incidence of multinodular thyroids, variable incidence of malignancy, variable approach to reporting and imaging of thyroids, and different attitudes to how to deal with the many false positive and some false negative results that will arise more frequently the more biopsies are done. What is an acceptable level of inaccuracy?
Many of the thyroid studies on ultrasound features of benign v malignant look at different populations, use different classification systems, and were done using different quality of equipment over the last twenty years. My current approach is heavily based on a large study published online August 26, 2013 in JAMA Internal Medicine (Dr. Rebecca Smith-Bindman et al at the University of California, San Francisco). This was a retrospective case-control study of patients who underwent thyroid ultrasound imaging from January 1, 2000, through March 30, 2005 and cross referencing with the California Cancer Registry. A total of 8806 patients underwent 11 618 thyroid ultrasound examinations during the study period, including 105 subsequently diagnosed as having thyroid cancer. Thyroid nodules were common in patients diagnosed as having cancer (96.9%) and patients not diagnosed as having thyroid cancer (56.4%). The researchers led by found that three ultrasound nodule characteristics were associated with thyroid cancer.
- Microcalcifications (odds ratio [OR], 8.1; 95% CI: 3.8-17.3) see figure 1
- Nodule size greater than 2 cm (OR, 3.6; 95% CI: 1.7-7.6) see figure 2
- An entirely solid composition (OR, 4.0; 95% CI: 1.7-9.2) see figure 3
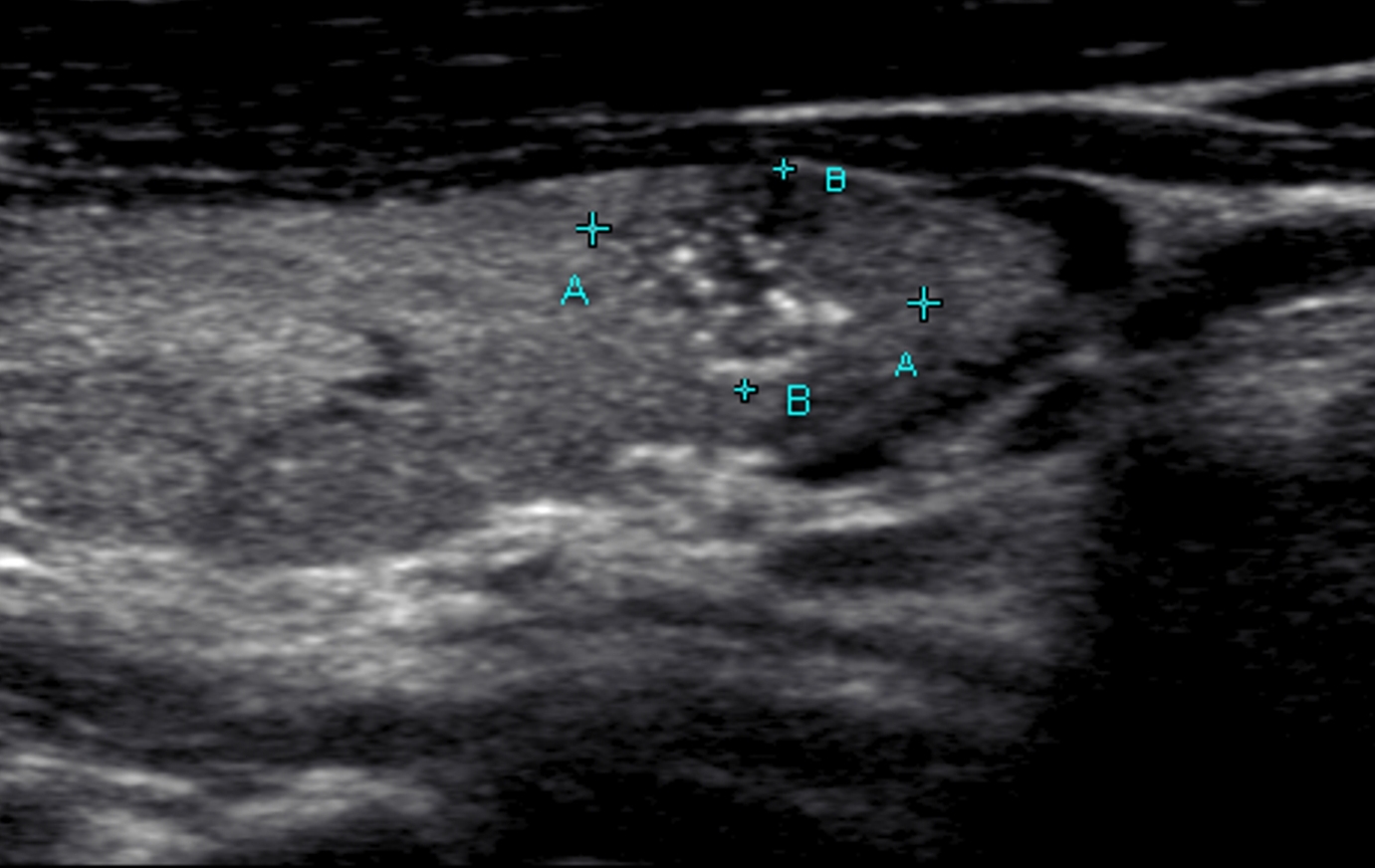
Figure 1. Thyroid microcalcifications commonly seen in papillary carcinoma

Figure 2. Example of a solid thyroid nodule
Requiring that two of these characteristics were present for a biopsy to be performed would dramatically reduce the number of unnecessary biopsies without missing many cancers, according to the findings.”If we restrict biopsy to those nodules that either have microcalcifications or are entirely solid and larger than 2 cm, we will find most cancers, and in patients in whom we don’t biopsy, the risk of cancer is quite low (< 0.5 per 100),” Smith-Bindman told AuntMinnie.com.
The study found that if 2 characteristics were required for biopsy, the sensitivity and false-positive rates would be lower (sensitivity, 0.52; 95% CI, 0.42-0.62; false-positive rate, 0.07; 95% CI, 0.07-0.08), the positive likelihood ratio would be higher (7.1; 95% CI, 6.2-8.2), and only 16 biopsies will be performed per cancer diagnosed. Compared with performing biopsy of all thyroid nodules larger than 5 mm, adoption of this more stringent rule requiring 2 abnormal nodule characteristics to prompt biopsy would reduce unnecessary biopsies by 90% while maintaining a low risk of cancer (5 per 1000 patients for whom biopsy is deferred).
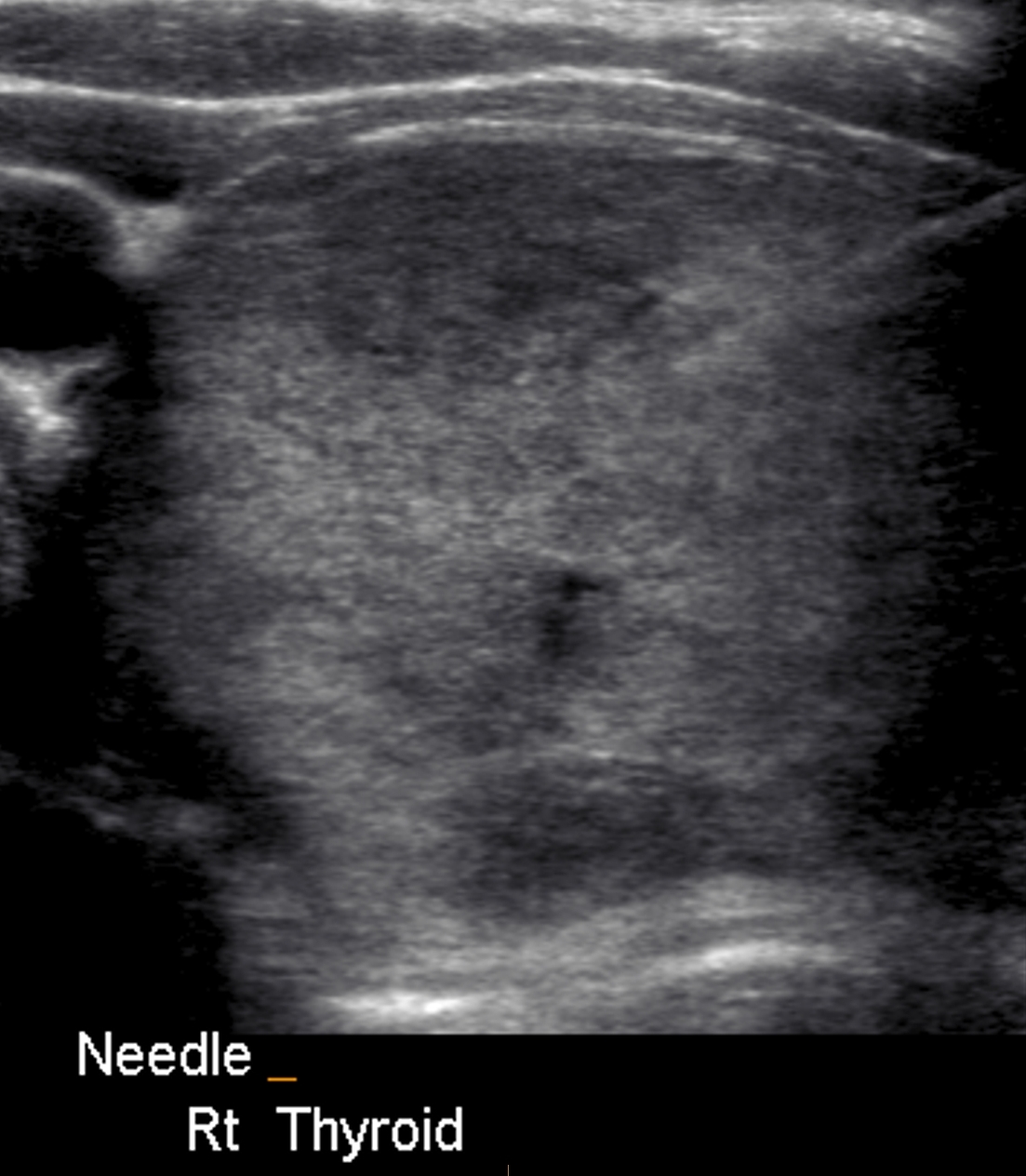
Figure 3. Large nodule undergoing a fine needle biopsy
“Most thyroid nodules are benign and do not need biopsy or surveillance,” Smith-Bindman told AuntMinnie.com. “Over 98% of thyroid nodules are benign. “Even for those with thyroid cancer, most have a favorable prognosis, with a 20-year survival rate greater than 97% even in patients who do not receive immediate treatment. “Given the favorable prognosis of most thyroid cancers even without treatment, a risk of cancer of 0.5% among those with a negative examination result seems to balance between detection and unnecessary tissue sampling,” the authors wrote. The researchers observed that the increased use and improved technical quality of ultrasound has led to detection of multiple morphologic characteristics, without clear criteria for what nodules need further treatment. This results in greater tissue sampling and excessive treatment, according to the group.
My own approach includes two further features not covered in the above study. One is a long long acknowledged as a risk factor of malignancy. If the patient has a nodule that is non-functioning on a thyroid nuclear scan then this finding can substitute for one of the features above. The second helps classify nodules larger than 2cm as benign but is only available on certain equipment and at more specialised centres: elastography. This is covered in another post, see Elastography.
Of course individual patient factors and wishes will occasionally over-ride these criteria and need to be taken into account (family history, radiation exposure, thyroid function tests, other imaging, clinical features, etc).
In summary I generally recommend a fine needle biopsy if two (or more) of the following imaging features are present:
-
Microcalcifications
-
Nodule size greater than 2 cm
-
An entirely solid composition
-
A score of 3 or higher on sonoelastography
-
Cold nodule on nuclear (pertechnetate) scan ( see figure 4)

Figure 4. Large cold nodule in right lobe of thyroid on nuclear scan.
UPDATE 2016 (For those of you who have requested more about ultrasound features and malignancy)
Recent studies have generally found four specific imaging features which differentiate between malignant and benign nodules. These are:
- Solid composition
- Hypoechogenicity
- Indistinct margin
- Taller than wide axis
- Abnormal elastography pattern
The presence of two of these features is sufficient to warrant a biopsy, regardless of the size of the lesion.
Further reading and information:
Incidental thyroid nodules are often found on patients having MRI,PET, or CT scans for other reasons. These should only be reported if they meet certain criteria –see Duke University 3 tiered system.
An excellent ULTRASOUND scoring system for determining management/classification of thyroid nodules is TIRADS (American College of Radiology Thyroid Imaging, Reporting and Data System). You can download a copy for personal use here.
Further information can be also be found at the American Thyroid Association website.
2021 Great new resource at https://tiro.expert/